
The Women's Health Collaborative and the AngioInstitute proudly presents an assembly of reports and clinical features produced by Dr. Noelle Cutter and her esteemed colleagues.
2024 UPDATES ON DENSE BREAST RESEARCH

This observational study explores the functional phenotypic differences that make dense breast tissue. Because it is widely noted that women with dense breasts have a greater likelihood of developing cancer, understanding the pathways and changes in gene expression may offer the first avenue for the enzymes enrolled and drug targets for personalized medicine in pursuit of developing better treatment options.
Day 1: Dr. Cutter is establishing the effectiveness of the tissue culture methods, indicating the capability of growing the cells. Working with epithelial cells that are growing at the expected density rate, she is able to start extracting DNA, RNA and proteins. By running functional analysis, the study allows for the observation of cell reaction from oxidative stress in the cell line. Additional information gathered include apoptosis (to monitor the cellular death) vs. general growth rate to understand their growth properties.
Day 2: Part of the functional analysis include the induction of environmental stress to provoke oxidative stress response to record cell endurance within breast cancer cell lines. Over 36 trials showed response to oxidative stress which could mimic inflammatory response from environmental stresses. Reports indicate continued cellular survival and that “they're happy to keep growing… without any change in cellular deaths”. Activating oxidative stress included: physically adding stressors such as hydrogen peroxide, serum‐starving and glucose‐starving the cells‐ all presenting the same response.


Cancers (Basel). 2020 Aug; 12(8): 2134.



Introduction:
SelectScience® Cancer Research Summit is celebrating its third year, bringing together the scientific community and pioneering manufacturers to foster collaboration and facilitate the dissemination of crucial updates in cancer research. Each year, scientific presentations by expert speakers deliver the latest findings in their respective topics, offering practical skills through engaging technology showcases, interactive resources by industry leaders- helping the community to harness the power of networking to drive impactful collaborations.
.webp) For the second year in a row, ICRS top clinical advocate Dr. Noelle Cutter was elected to be one of the headliners of this global (virtual) medical event. With her, she brought fellow cancer researchers and two powerhouse publishers in women's health- Dr. Robert L. Bard (Sr. Cancer Imaging Radiologist) and Dr. Roberta Kline (OBGYN/ Genomics Expert). Together, Dr. Cutter's presentation promises to empower the medical community with the most comprehensive report on "Molecular Changes in Dense Breast Tissue" and its metabolic correlation with Breast Cancer.
For the second year in a row, ICRS top clinical advocate Dr. Noelle Cutter was elected to be one of the headliners of this global (virtual) medical event. With her, she brought fellow cancer researchers and two powerhouse publishers in women's health- Dr. Robert L. Bard (Sr. Cancer Imaging Radiologist) and Dr. Roberta Kline (OBGYN/ Genomics Expert). Together, Dr. Cutter's presentation promises to empower the medical community with the most comprehensive report on "Molecular Changes in Dense Breast Tissue" and its metabolic correlation with Breast Cancer.
This video presentation is comprised of 3 presentations which can be accessed in full assembly or as separate clips: (1) Dr. Noelle Cutter -part 1 (2) Dr. Robert Bard (3) Dr. Roberta Kline (4) Dr. Noelle Cutter - Part 2. Scroll below for direct access to all presentations and transcripts.

Breast cancer is the most common cancer worldwide, recently surpassing lung cancer in 2020. Globally, it is the number one cancer in both developed and underdeveloped countries and affects more than 2.3 million people, both men and women worldwide, despite its global abundance. Knowledge about the first steps in tumor initiation is important for early detection. However, the exact mechanisms of tumor initiation are still unknown. The median age of diagnostics is 62 to 63 years old, but more recent data also shows that breast cancer is the most common type of cancer among young women.

TRIBUTE TO A GLOBAL CRUSADER (Play Video-L) The NY Cancer Resource Alliance gives loving tribute to Dr. Nancy Cappello, co-founder of "Are You Dense" and chief crusader of the mission to bring change to the protocols and standards of Early Detection. Her organization embarked in a global advocacy project to win legislation for dense breast scanning and to bring awareness to the need for better technologies and imaging interpretation. Today, her loving husband Joe continues her unending fight to save more lives through awareness, advocacy and her crusade for change. (Also see below to read her full story in our ORG SPOTLIGHT section) |
<
Molecular profiling of gene expression of breast cancers has demonstrated that tumors are remarkably heterogeneous. More recently, molecular analysis of the microenvironment has demonstrated similar heterogeneity, but the epidemiological clinical and pathological correlations of this variation are not well studied. Recent advances of breast cancers and the surrounding and microenvironment have revealed important stromal and epithelial interaction and have led to the speculation that the microenvironment may actually be dominant over tumor biology, especially early in the stage of progression when invasive cancer cells are still forming.

We used a subset of genes quantified by the cancer genome atlas, which represent copy number variation where the CNV is low and downregulation of gene expression is seen, or we can look at copy number variations and gene upregulation for our functional genomic study. We next correlated this data to methylation changes across the genome using a platform known as MoMA, which is a methylation detection array. The image presented represents a sample representation of the heat met, which included 749 differentially methylated probes showing the segregation of mammographically dense and non mammographically dense patients with breast cancer. Since this analysis is based on the comparison of the two co cohorts of mammographically dense and non mammographically dense, there are regions that are found more frequently methylated in mammographically dense or non mammographically dense, breaking down to approximately 60% methylated in mammographically dense and 40% methylated in non mammographically dense tumors. For these regions that differentiate between the mammographically dense and non mammographically dense, we next determine which methylation event potentially represses transcription.

When we analyze our subset of genes identified by the cancer genome atlas and shared publicly that are differentially expressed in patients with breast cancer and high mammographic density, we then uploaded our methylation gene list to a bioinformatic platform known as David to help identify any enriched themes in um, biological functionality for the subset of our genes. The David platform is the database for annotation visualization and integrated discovery and provides a comprehensive set of functional annotation tools for investigators to understand the biological meaning behind some of the large gene lists, such as the one that we isolated for our mammographically dense and our non mammographically dense patients. The star on the slide indicates pathways that are currently under validation in our lab and the hashtag indicates publications that have already been accepted for our gene analysis. That list.

Our studies have shown that gene expression upregulation of these two key genes, ZB one and TNF Alpha, also induced functional changes in our cell lines, which include cellular proliferation and invasion. Being that TNF alpha and ZB one promote cell displacement and invasive myth through that EMT pathway, we hear and propose that these genes employ a pathogenic mechanism to render mammographically dense cells to metastasize. EMT is an overly complex but also reversible event. Therefore, further investigation into these genes in the an inhibition of either TNF alpha or Zev one might be an effective strategy for personalized medicine and cancer therapy.


Material Disclosure: Except as expressly set forth herein, as between the Parties, each Party is and shall remain the owner of all intellectual property that it owns or controls as of the effective date 11/1/2023 or that it develops or acquires thereafter. This information including all images and statements presented herein are submitted under limited license and are copyrights held and maintained by the speakers/producers of each segment and are protected under U.S. and international copyright laws adhering all intellectual properties. All content and intended solely for the attention and use of the recipient of the email with which this document is attached. This information is protected by work product privilege or other legal rules. It must not be disclosed to any person without our authority or published, posted or shared to other parties unknown in any way.
WOMEN’S HEALTH COLLABORATIVE GOES TO ALBANY
Friday, May 10, 2024
NEWS RELEASE: The National Coalition for Ultrasound Screening


In a recent “Cancer Powermeet” event, leading advocacy leader Ms. Barish joined the WHC concept about “EARLIER DETECTION” in support of proactive screenings for women from 20-39. “Due to the continuing rise in numbers of breast cancer cases in younger women, doctors need to change their thinking about starting checkups at 40.” Innovative screening plans comprise the use of ultrasound in screening centers and traveling vans as a starting point in underserved locations. For over 20 years, Ms. Barish has been active in state congress about a list of cancer related interests impacting women’s health including public initiatives like environmental causes and legislative change in healthcare protocols.

The outreach team behind the WHC aims to connect with lawmakers and health professionals alike, in pursuit of change through awareness. The Women’s Health Collaborative continues its mission to unite with new resources in support of better screening, community outreach and educational efforts to improve healthcare for women.

PROGRAM 1: EARLIER DETECTION


Tuesday, September 19, 2023
A NEED TO STANDARDIZE SCREENING WITH DENSE BREAST SCANNING
What Does It Mean to Have Dense Breasts?

 BREAST CANCER RISK: Women with dense breasts have a higher chance of getting breast cancer. The more dense your breasts are, the higher your risk. Scientists don’t know for sure why this is true. Breast cancer patients who have dense breasts are not more likely to die from breast cancer than patients with non-dense (fatty) breasts.
BREAST CANCER RISK: Women with dense breasts have a higher chance of getting breast cancer. The more dense your breasts are, the higher your risk. Scientists don’t know for sure why this is true. Breast cancer patients who have dense breasts are not more likely to die from breast cancer than patients with non-dense (fatty) breasts.
Tuesday, September 28, 2021
Dense Breast Research: Code name IRON-WOMAN
Research overview: MAMMOGRAPHIC DENSITY, PHYSICAL ACTIVITY AND BREAST CANCER
Written by: Dr. Noelle Cutter / Sept. 12, 2021
Edited by: the publishing team @ NYCRANEWS.com
Mammography, as the primary screening modality, has facilitated a substantial decrease in breast cancer-related mortality in the general population. However, the sensitivity of mammography for breast cancer detection is decreased in women with higher breast densities, which is an independent risk factor for breast cancer. With increasing public awareness of the implications of a high breast density, there is an increasing demand for supplemental screening in these patients. Yet, improvements in breast cancer detection with supplemental screening methods come at the expense of increased false-positives, recall rates, patient anxiety, and costs. Therefore, breast cancer screening practice must change from a general one-size-fits-all approach to a more personalized, risk-based one that is tailored to the individual woman's risk, personal beliefs, and preferences, while accounting for cost, potential harm, and benefits.
FACTOIDS & FIGURES- The Inspiration behind our research initiative [1]:
▪ Breast cancer is the second most common cancer among women in the United States and about 1 in 8 U.S. women (about 13%) will develop invasive breast cancer over the course of her lifetime.
▪ In 2021, it is estimated that over 280,000 new cases of invasive breast cancer will be diagnosed in women in the U.S.,
▪ Over 40,000 women in the U.S. are expected to die in 2021 from breast cancer. Unfortunately, death rates have been steady in women under 50 since 2007, despite advancements in treatment options.
▪ For women in the U.S., breast cancer death rates are higher than those for any other cancer, besides lung cancer.
▪ As of January 2021, there are more than 3.8 million women with a history of breast cancer in the U.S. This includes women currently being treated and women who have finished treatment.
▪ Breast cancer is the most commonly diagnosed cancer among American women. In 2021, it's estimated that about 30% of newly diagnosed cancers in women will be breast cancers.
▪ Breast cancer became the most common cancer globally as of 2021, accounting for 12% of all new annual cancer cases worldwide, according to the World Health Organization.
▪ A woman’s risk of breast cancer nearly doubles if she has a first-degree relative (mother, sister, daughter) who has been diagnosed with breast cancer.
 |
| Click for full lecture with Dr. N. Cutter & Dr. L. Bard |
▪ About 85% of breast cancers occur in women who have no family history of breast cancer.
The most significant risk factors for breast cancer are sex (being a woman) and age. But recent research is beginning to clarify additional risk factors associate with BC
PHYSICAL ACTIVITY
Physical activity is considered a significant modifiable factor in breast cancer risk, and since exercise reduces fatty tissue and BMI, it has been thought to increase breast density. However, studies into the relationship between physical activity and breast density have been inconclusive. Other factors such as alteration in metabolism of endogenous hormones, are suggested to influence mammographic density (MD) as well. Therefore, it is evident that the links between physical activity and breast cancer risk need to be clarified.
BREAST TISSUE DENSITY
Breast density levels refer to the appearance of the breast tissue on a mammogram. Breast density is part of the supportive or connective tissue that makes up the breast tissue. As you can see in this image, breast tissue is white to gray and transparent against a dark background. Denser breast tissue appears more white whereas fatty/non-dense tissue appears grapy and transparent.
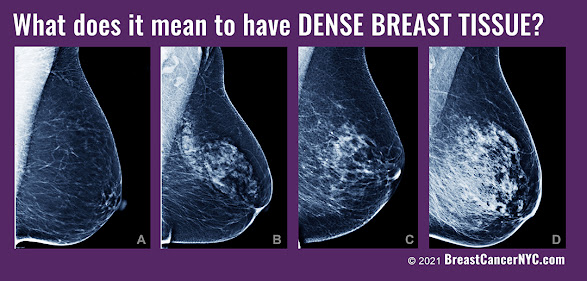
Levels of density are described using a results reporting system called Breast Imaging Reporting and Data System (BI-RADS). The levels of density are often recorded in your mammogram report using letters. The levels of density are:
A: Almost entirely fatty indicates that the breasts are almost entirely composed of fat. About 1 in 10 women has this result.
B: Scattered areas of fibroglandular density indicates there are some scattered areas of density, but the majority of the breast tissue is non-dense. About 4 in 10 women have this result.
C: Heterogeneously dense indicates that there are some areas of non-dense tissue, but that the majority of the breast tissue is dense. About 4 in 10 women have this result.
D: Extremely dense indicates that nearly all of the breast tissue is dense. About 1 in 10 women has this result.
In general, women with breasts that are classified as heterogeneously dense or extremely dense are considered to have dense breasts. Almost half of women undergoing mammograms have dense breasts.
A close up here shows the difference in imaging for a breast tumor on non-dense vs dense breast tissue using a mammogram. Breast density has been widely considered a strong risk factor for breast cancer, with statistics suggesting as much as a six times higher likelihood of the disease in breasts, compared with those with a less dense breast tissue. Not only does dense breast tissue make it harder for a mammogram to pick up small tumors, but dense breasts themselves have been associated with a higher chance of cellular abnormality.

Women who have dense breast tissue have a higher risk of breast cancer compared to women with less dense breast tissue. It’s unclear at this time why dense breast tissue is linked to a higher lifetime risk of breast cancer. Understanding that link is extremely important.
Dense breast tissue also makes it harder for radiologists to see cancer. On mammograms, dense breast tissue looks white. Breast masses or tumors also look white, so the dense tissue can hide tumors. But fatty tissue looks almost black. On a black background it’s easier to see a tumor that looks white. So, mammograms can be less accurate in women with dense breasts.
One of the challenges in promoting the widespread utility of breast cancer risk prediction models has been the assertion that most women with a diagnosis of breast cancer have no established clinical breast cancer risk factors or are not considered to be high risk. [1][2] Although it is impossible to determine the cause of breast cancer in any individual case [3] easily assessed risk factors that explain a substantial proportion of incident breast cancers can be used to stratify breast cancer risk for targeted screening [4] and primary prevention [5] and improve public health interventions to reduce breast cancer risk.
Recent research has suggested that for women with dense breasts, a screening strategy that also takes into account a woman’s risk factors and protective factors may be the best predictor of whether a woman will develop breast cancer after a normal mammogram and before her next scheduled mammogram.

Breasts contain glandular, connective, and fat tissue. Breast density is a term that describes the relative amount of these different types of breast tissue as seen on a mammogram. Dense breasts have relatively high amounts of glandular tissue and fibrous connective tissue and relatively low amounts of fatty breast tissue.
HOW COMMON ARE DENSE BREASTS?
Nearly half of all women age 40 and older who get mammograms are found to have dense breasts. Breast density is often inherited, but other factors can influence it. Factors associated with lower breast density include increasing age, having children, and using tamoxifen. Factors associated with higher breast density include using postmenopausal hormone replacement therapy and having a low body mass index.
Women with dense breasts have a higher risk of breast cancer than women with fatty breasts, and the risk increases with increasing breast density. This increased risk is separate from the effect of dense breasts on the ability to read a mammogram. MD one of the strongest risk factors. And because individuals with denser breasts tend to develop more serious types of breast cancer, understanding the connection is important.

A common question that invariably comes up when discussing breast density relates to breast density in athletes. As an athlete myself who has dense breasts, I was struck by the number of individuals in my athletic community who also have dense breasts. A shocking trend was seen in the overwhelming amount of young women with dense breasts who subsequently had received false negative mammogram reports.
What we do know is that your breast tissue tends to become less dense as you age, though some women may have dense breast tissue at any age. Women with less body fat are more likely to have more dense breast tissue compared with women who are obese. From observation (thus far), athletic women are also more likely to have dense breast tissue. One of the main goals of our study is to really try to understand the biological connection of breast density in athletes as well as run a retrospective study on how common this trend is.
RESEARCH OBJECTIVES
It's not clear why some women have a lot of dense breast tissue and others do not. You may be more likely to have dense breasts if you:
▪ ARE YOUNGER; your breast tissue tends to become less dense as you age, though some women may have dense breast tissue at any age.
▪ HAVE LOWER BMI (body mass index); women with less body fat are more likely to have more dense breast tissue compared with women who are obese.

Although breast density is a well-established, strong, and prevalent breast cancer risk factor it’s biological connection is not clearly understood. More research is needed to support the population associated risk proportion in athletic pre-menoposal women. Our data will start with a cohort of women undergoing imaging ultrasounds at the Bard Cancer Diagnostic Center. Our population will include pre-menoposal women with dense breasts.
METHODS
Endurance athletes are defined those who participated in one or more endurance events (long course) in the year or as well as those who are (younger, low BMI cohort). MD and classification of “dense breasts” was heterogeneous and extremely dense as noted by the BI_RADS code; (heterogeneously or extremely dense vs scattered fibroglandular densities). Data will be collected as odds ratio (OR’s) and 95% confidence intervals included in our outcomes
Cross-sectional Analysis | 1000+ pre-menopausal women aged 18+ |
Collect information on height, weight, BMI and history of disease | Physical activity assessment |
MD measurement performed by radiologist and confirmed by ultrasound | Logistic regression used to estimate the association of MD within participation in physical activity |

JAMA STUDY:
A recent report in Journal of the American Medical Association found that first-degree family history of breast cancer dense breasts were associated with an increased population associated risk proportion of breast cancer. Among premenopausal women, the largest individual population associated risk proportion was for breast density, with 28.9% (95% CI, 25.3%-32.5%) of breast cancers potentially removed by reducing breast density from BI-RADS heterogeneously or extremely dense breasts to scattered fibroglandular densities. The population associated risk proportion for breast density increased to 65.5% (95% CI, 60.4%-70.6%) if all premenopausal women reduced their breast density to the lowest category of almost entirely fat tissue.
SUMMARY/ WRAP-UP
Given that greater breast density as categorized by the BI-RADS remains a factor associated with breast cancer for all ages of women, information about breast density together with life expectancy may benefit clinical decision-making regarding screening. In March 2019, the US Food and Drug Administration recommended changes to the Mammography Quality Standards Act to make it mandatory to report breast density information to both patients and their physicians. However, how women and their physicians should use this information to inform screening recommendations is unclear. Very dense breasts may increase the risk that cancer won't be detected on a mammogram.
What is clear is that additional research is needed to elucidate the mechanisms underlying the observed associations between breast density and risk of breast cancer. As newer and more advanced breast density assessment techniques are developed, evaluation of the diffusion of such innovations with an aim of developing individualized screening strategies will be important, particularly among athletic women, for whom dense breast are more likely seen.

EPILOGUE

With your support, we are able to implement this screening program for women's health as well as help fund this clinical research. Our work will advance technology, change legislation and most importantly save lives through awareness.
Wednesday, July 7, 2021
Ultrasound Significantly Reduces False Readings of DENSE BREASTS

What Does It Mean to Have Dense Breasts?


