Written by: Lennard M. Goetze, Ed.D / Robert L. Bard, MD
DR. MARK LEBWOHL, a distinguished figure in dermatology and Dean for Clinical Therapeutics at Mount Sinai, recently shared insights into groundbreaking research and innovations in dermatological care. His extensive contributions have transformed the field, particularly in inflammatory skin diseases, neurocutaneous conditions, and skin cancer diagnostics.
BREAKTHROUGHS IN DERMATOLOGY
Mount Sinai's dermatology research team is at the forefront of significant advancements. Dr. Brian Kim has been leading efforts in neurocutaneous symptoms, particularly in alleviating severe itching. His work continues to produce transformative discoveries, improving patient outcomes significantly.
Dr. Emma Guttman has revolutionized the understanding and treatment of alopecia areata, identifying its autoimmune causes and pioneering targeted therapies. Her research has shifted paradigms in dermatology, leading to safer and more effective treatments for hair loss, atopic dermatitis, and other immune-related skin disorders. One of her most notable achievements is the development of dupilumab, a drug that has benefited hundreds of thousands suffering from eczema. Her work has further extended into conditions like bullous pemphigoid, hand dermatitis, nummular eczema, and urticaria. "Our studies at Mount Sinai constantly lead to breakthrough discoveries that are translated to better patient care for patients with inflammatory skin diseases", states Dr. Guttman.
Innovations in Psoriasis and Vitiligo Treatment
The Mount Sinai team has also been at the cutting edge of psoriasis research, focusing on pustular psoriasis and pyoderma gangrenosum, two devastating conditions. Their ongoing efforts continue to refine treatments that dramatically improve patients’ lives. In the realm of vitiligo, they have challenged misconceptions that dismiss it as merely cosmetic. Instead, they highlight its deep psychological impact, particularly in patients with darker skin tones. Current therapies show promise in re-pigmenting skin, though the team continues to strive for faster and more effective solutions.
Leading Clinical Trials and Expanding Research
Dr. Lebwohl has played a pivotal role in expanding Mount Sinai’s clinical trials, aiming to introduce safer and more effective dermatological treatments. His leadership has helped establish one of the largest dermatology clinical trials units in the country, bringing new drugs to market that significantly improve patient care. His recruitment of Dr. Emma Guttman has further enhanced Mount Sinai’s research capabilities, securing extensive funding from both government and pharmaceutical sources.
Their investigations extend beyond inflammatory conditions into neurocutaneous disorders, squamous cell carcinoma, and melanoma. Mount Sinai offers unmatched diagnostic tools, including optical coherence tomography, confocal microscopy, and total body imaging using the Vectra system, setting a global benchmark for skin cancer detection.
Cutting-Edge Diagnostic Imaging and AI Integration
In dermatological diagnostics, advanced imaging plays a crucial role. Technologies like confocal microscopy and electrical impedance analysis aid in early cancer detection. The Vectra total body imaging system, one of the few available in the U.S., enables precise mole mapping, identifying changes that could indicate malignancy.
Artificial intelligence is also beginning to shape dermatology. AI-assisted diagnostics can analyze skin lesions and biopsy results, complementing the expertise of dermatopathologists. While AI will never replace doctors, it serves as a valuable tool, especially in identifying skin cancers and streamlining insurance approvals for life-changing medications.
First Responders and Skin Cancer Risks
Mount Sinai investigators have identified the increased risk of skin cancer among first responders, attributing it to heightened sun exposure and potential environmental toxins. Mount Sinai’s dedicated program for first responders has identified a significant number of skin cancer cases, underscoring the importance of routine screenings and preventive measures.
Philanthropy and Future Directions
Dr. Lebwohl has been instrumental in securing funding for research initiatives. His efforts led to the establishment of the Mark Lebwohl Center for Neuroinflammation and Sensation, dedicated to advancing treatments for conditions like chronic itch. While humbled by the recognition, he remains focused on developing novel therapies and ensuring Mount Sinai remains a global leader in dermatology.
Conclusion
Dr. Mark Lebwohl and his colleagues at Mount Sinai continue to push the boundaries of dermatological research. Their pioneering work in inflammatory skin diseases, advanced imaging, AI integration, and clinical trials is transforming the landscape of dermatology, offering patients renewed hope and better quality of life. As they forge ahead, their commitment to scientific discovery ensures that dermatology remains at the forefront of medical innovation, improving lives worldwide.
Eye on Medical Innovations:
WOUND HEALING & the ARTIFICIAL SKIN
By definition, WOUND HEALING refers to the regeneration of damaged or destroyed skin/tissue by newly produced tissue. Upon a traumatic event to the body causing a breach or tear in the epithelial layer, a national and expected cascade of biochemical events is activated to repair the damage to form a protective barrier from the outside environment. This is our body's way of protecting itself from infection, bacteria or further injury. The process of wound-healing may encounter unforeseen failure in its natural regenerative process, leading to chronic disease and further wounds (ie. diabetic wounds or diabetic ulcers). This can lead to more serious infections and reinjury. BARDDIAGNOSTICS has joined the technological movement to advance wound healing science through real-time 3D ultrasound monitoring and laser thermographics. This aids the mitigation of the wound recovery process by immediately identifying the depth of the injury and the extent of the damage (neurological, vascular, circulatory) underneath. (see complete feature). Also see: "Researching Exosomes for Skin Disorders".
First Responders Cancer: Inspiring a Global Diagnostic Upgrade
It has been confirmed by toxicologists and medical reports worldwide that OCCUPATIONAL HEALTH DISORDERS are predominant in the fire service. First responders hold potential cancer risks from the most extreme toxic exposures in every fire rescue call. My diagnostic practice (in mid-town NYC) provided care for many first responders from 9/11 as well as current active duty firefighters. For those with low grade tumors, yearly monitoring with sonograms is a safe and easy solution- agreeing to be biopsied only when a significant change is noted in comparison. Thanks to non-invasive diagnostics, men relying on alternative treatments would come in to check if their “natural products” were helping. Experience showed over 50,000 scans since 1974 identified low grade cancer (Gleason 3+3) turns aggressive in less than 1% over a 10 year time frame.
The radiology community took time to appreciate that pathologic cancer tissue under microscope can be clinically dormant with some patients. This means a biopsy that looks like malignancy can act like a chronic disease. New high resolution ultrasound units and computerized optical devices are now used instead of MRI for diagnosing Prostate Cancer in Europe and guiding biopsies without x-rays. MRI has shown to be less accurate in the upper and lower parts of the prostate gland and has a 33% false positive rate in the presence of inflammation. When the sonogram finds prostatitis, MRI is deferred until the infection is resolved.
From our experience working with the many first responder cases, we have been alerted to the greatly increased risk of cancer following toxic exposure. Surprisingly, first responders are developing prostate and skin cancers at a higher rate than lung cancer. New portable sonogram systems are able to find and quantify the heavy metal effects on the skin in a 5 minute exam which is now called ULTRASOUND BIOMICROSCOPY. This is important since tissue under a microscope is not living while sonogram technology gives a live tissue real-time virtual biopsy.
What makes for added concern are the numerous WHITE DOTS (calcific foci) surrounding the dark area which are micro-calcifications, otherwise called testicular microlithiasis (TM) or micro-stones. According to a 2018 study, this uncommon condition of micro-stones is linked to testicular cancer (as well as male infertility) possibly increasing one's risk as much as 1200%. While not technically a precancerous condition, any man with these microcalculi should be checked periodically whereby small tumors could be treated focally if caught early. Since this 9mm tumor cannot be felt by itself, the simplest way to accurately identify the cause of the enlarged testis is with a high resolution sonogram. This non invasive screening may be also recommended for male family members. (See complete article)
Disclaimer & Copyright Notice: Copyright (c) 2021, IntermediaWorx inc. All Rights Reserved. Additional copyrights shared by: The AngioFoundation (501c3) and the publishers of Prevention101.org & The NY Cancer Resource Alliance [NYCRAlliance.org]. Contents in this article are provided publicly for informational purposes within non-commercial use and not for purposes of resale, distribution, commercial display or performance. Unless otherwise indicated on this web based page, no reproduction of any or all materials of this page is allowed without express/written permission from the publishers. Additional permission may be required from third-parties who have provided limited permission for our publishers to use their content, whereas licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.
The Women's Health Collaborative and the AngioInstitute proudly presents an assembly of reports and clinical features produced by Dr. Noelle Cutter and her esteemed colleagues.
2024 UPDATES ON DENSE BREAST RESEARCH
3/6 ‐ 3/8/2024 ‐Molloy University Labs, NY. Dr. Noelle Cutter works with live breast cancer cells in dense breast tissue (Adenocarcinoma, breast, epithelial ER+ ‐estrogen receptor expressed).
This observational study explores the functional phenotypic differences that make dense breast tissue. Because it is widely noted that women with dense breasts have a greater likelihood of developing cancer, understanding the pathways and changes in gene expression may offer the first avenue for the enzymes enrolled and drug targets for personalized medicine in pursuit of developing better treatment options.
Day 1: Dr. Cutter is establishing the effectiveness of the tissue culture methods, indicating the capability of growing the cells. Working with epithelial cells that are growing at the expected density rate, she is able to start extracting DNA, RNA and proteins. By running functional analysis, the study allows for the observation of cell reaction from oxidative stress in the cell line. Additional information gathered include apoptosis (to monitor the cellular death) vs. general growth rate to understand their growth properties.
Day 2: Part of the functional analysis include the induction of environmental stress to provoke oxidative stress response to record cell endurance within breast cancer cell lines. Over 36 trials showed response to oxidative stress which could mimic inflammatory response from environmental stresses. Reports indicate continued cellular survival and that “they're happy to keep growing… without any change in cellular deaths”. Activating oxidative stress included: physically adding stressors such as hydrogen peroxide, serum‐starving and glucose‐starving the cells‐ all presenting the same response.
Senescence in Dense Breast Tissue: A Functional Role for Metastasis By: Noelle L. Cutter, PhD
Studies show that persistent populations of senescent cells can use senescence as an adaptive pathway to restart proliferation and become more aggressive. These are our dense breast cells. The blue ones are senescent cells.
Senescence, the state of irreversible growth arrest, has been proposed to play a role in the metastasis of dense breast tissue. Dense breast tissue is characterized by a higher proportion of glandular and connective tissue compared to fatty tissue. Studies suggest that dense breast tissue provides a conducive environment for cancer cells to thrive and metastasize.
One proposed mechanism involves senescent cells secreting factors that can promote tumor growth and metastasis. These factors include pro-inflammatory cytokines, growth factors, and extracellular matrix remodeling enzymes. Senescent cells can also alter the tissue microenvironment, making it more favorable for the survival and dissemination of cancer cells.
Additionally, senescent cells may escape the immune system's surveillance, allowing them to persist in the tissue and contribute to tumor progression. The accumulation of senescent cells in dense breast tissue over time may create a pro-tumorigenic milieu, facilitating the initiation and spread of cancer cells.
Furthermore, senescent cells have been implicated in promoting angiogenesis, the formation of new blood vessels, which is crucial for tumor growth and metastasis. By secreting angiogenic factors, senescent cells can stimulate the formation of blood vessels that supply nutrients and oxygen to the growing tumor, facilitating its expansion and dissemination to distant sites.
Overall, the proposed role of senescence in dense breast tissue metastasis involves creating a tumor-promoting microenvironment, facilitating immune evasion, and promoting angiogenesis, all of which contribute to the progression and spread of cancer cells. However, further research is needed to fully elucidate the mechanisms underlying this process and to explore potential therapeutic strategies targeting senescent cells in the context of breast cancer metastasis.
NOELLE CUTTER, PhD - Associate professor in higher education in biology and chemistry, lover of technology and learning. Motivational speaker focused on student success. Ironman athlete. Data enthusiast. United with an expanding research team dedicated to collecting data on women with dense breasts and screening options for these patients, her initiative aims to investigate and gather conclusive information about dense breasts in specific groups- including age, body mass index, and amount of physical activity and the underlying diagnostics of breast cancer tumors. This research program is under a partnership with Molloy Univ. and Dr. Robert Bard, expert diagnostic cancer imaging specialist in NYC and other colleagues from the NY Cancer Resource Alliance.
Intl. Cancer Research Summit 2023@ Multi-Expert Presentation Panel
The following is a presentation from the SELECTSCIENCE Cancer Research Summit 2023 (on Nov. 14. 2023): exploring the latest developments in cancer research with fellow scientists, manufacturers, and regulatory experts
Introduction: SelectScience® Cancer Research Summit is celebrating its third year, bringing together the scientific community and pioneering manufacturers to foster collaboration and facilitate the dissemination of crucial updates in cancer research. Each year, scientific presentations by expert speakers deliver the latest findings in their respective topics, offering practical skills through engaging technology showcases, interactive resources by industry leaders- helping the community to harness the power of networking to drive impactful collaborations.
For the second year in a row, ICRS top clinical advocate Dr. Noelle Cutter was elected to be one of the headliners of this global (virtual) medical event. With her, she brought fellow cancer researchers and two powerhouse publishers in women's health- Dr. Robert L. Bard (Sr. Cancer Imaging Radiologist) and Dr. Roberta Kline (OBGYN/ Genomics Expert). Together, Dr. Cutter's presentation promises to empower the medical community with the most comprehensive report on "Molecular Changes in Dense Breast Tissue" and its metabolic correlation with Breast Cancer.
Hi everybody. I'm coming to you from Molloy University where in my lab, we study molecular changes in breast cancer. Joining me today, I have Dr. Robert Bard and Dr. Roberta Kline. Dr. Bard is an internationally recognized leader in the field of 21st century 3D ultrasonic volumetric doppler imaging. Dr. Bard specializes in advanced 3D sonography to detect cancers in numerous organs including the breast. Also with us is Dr. Roberta Kline, a board certified OB GYN Air Force veteran and a functional genomics and mind-body expert. She bridges conventional and alternative worlds to harness the best technologies and knowledge to create better health.
The complexity of cancer can be reduced to a small number of underlying principles, all share common traits or hallmarks that govern transformation of normal cells to malignant cells. The famous Hanahan and we Weinberg paper was redesigned since its first publication back in 2001. The latest publication in 2022 included non mutational, epigenetic reprogramming and global changes in the epigenetic landscape are now recognized as a feature of many cancers.
Breast cancer is the most common cancer worldwide, recently surpassing lung cancer in 2020. Globally, it is the number one cancer in both developed and underdeveloped countries and affects more than 2.3 million people, both men and women worldwide, despite its global abundance. Knowledge about the first steps in tumor initiation is important for early detection. However, the exact mechanisms of tumor initiation are still unknown. The median age of diagnostics is 62 to 63 years old, but more recent data also shows that breast cancer is the most common type of cancer among young women.
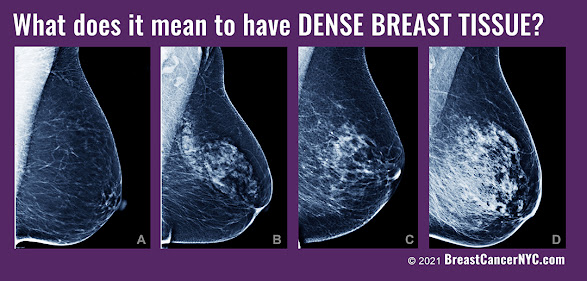
Ages 15-39 accounting for 30% of all cancers in this age group, understanding both the genetic and environmental makeup of the cancer will help drive better treatment for our patients. Mammographic density captured on film screen mammograms refers to the content and architectural structure of adipose, connective and epithelial tissues of the breast. In epidemiological studies, a high percentage of mammographic density confers up to a four to sixfold elevated risk of developing breast cancer. Mammographic density is to a large degree in inherited trait, although it is influenced by environmental factors as well. Levels of density are described using a reporting system called the Breast Imaging Reporting and Data System known as birads. The levels of density are a almost entirely fatty, which indicates that the breasts are almost entirely composed of fat. About one in 10 women have this result.
Fig-B (R) shows scattered areas of fibro-glandular density, which indicates that there are some scattered areas of density, but most of the breast tissue is non dense. About four in 10 women will have this result. Heterogeneously dense indicates that there are some areas of non dense tissue, but that most of the breast tissue is considered dense. About four in 10 women will have this result. Extremely dense indicates that nearly all of the breast tissue is considered dense. About one in 10 women have this result. This slide shows a box plot for mammographic density and breast cancer subtypes. Um, the percentage of mammographic density tumors in each of the subtypes are shown for basal HER2, LumA, LumB, and normal. (to be continued below)
TRIBUTE TO A GLOBAL CRUSADER
(Play Video-L) The NY Cancer Resource Alliance gives loving tribute to Dr. Nancy Cappello, co-founder of "Are You Dense" and chief crusader of the mission to bring change to the protocols and standards of Early Detection. Her organization embarked in a global advocacy project to win legislation for dense breast scanning and to bring awareness to the need for better technologies and imaging interpretation. Today, her loving husband Joe continues her unending fight to save more lives through awareness, advocacy and her crusade for change. (Also see below to read her full story in our ORG SPOTLIGHT section)
TRANSCRIPT & VISUAL PRESENTATION
By: Dr. Noelle Cutter(Part 2)
<
Molecular profiling of gene expression of breast cancers has demonstrated that tumors are remarkably heterogeneous. More recently, molecular analysis of the microenvironment has demonstrated similar heterogeneity, but the epidemiological clinical and pathological correlations of this variation are not well studied. Recent advances of breast cancers and the surrounding and microenvironment have revealed important stromal and epithelial interaction and have led to the speculation that the microenvironment may actually be dominant over tumor biology, especially early in the stage of progression when invasive cancer cells are still forming.
Clinical questions we ask in the lab are centered around identification of genetic signatures in that microenvironment of patients with dense breasts. If we can identify molecular changes, we can identify targets that are druggable using publicly available data to identify subsets of genes that are differentially expressed in breast cancer and correlated with high mammographic density. To identify important biological pathways is one of the methods that we've been utilizing in our labs. Um, using a bioinformatic parameter, we wanted to establish an in vitro, invitro 3D cell culture analysis that will accurately represent mammographic density. We are also interested in studying how gene suppression can be mimicked through the epigenetic mechanism of methylation. The methylation should induce suppression of transcription factors and that can be modeled within our in vitro system using a CRISPR Cas nine system. Once introduced into the cells growth characteristics and functional features can be studied. We propose that the analysis of these candidate genes that are identified in our study will help physicians make better clinical decisions when treating their patients.
We used a subset of genes quantified by the cancer genome atlas, which represent copy number variation where the CNV is low and downregulation of gene expression is seen, or we can look at copy number variations and gene upregulation for our functional genomic study. We next correlated this data to methylation changes across the genome using a platform known as MoMA, which is a methylation detection array. The image presented represents a sample representation of the heat met, which included 749 differentially methylated probes showing the segregation of mammographically dense and non mammographically dense patients with breast cancer. Since this analysis is based on the comparison of the two co cohorts of mammographically dense and non mammographically dense, there are regions that are found more frequently methylated in mammographically dense or non mammographically dense, breaking down to approximately 60% methylated in mammographically dense and 40% methylated in non mammographically dense tumors. For these regions that differentiate between the mammographically dense and non mammographically dense, we next determine which methylation event potentially represses transcription.
DNA methylation is an important epigenetic modification that defines the properties of cells. Genome-wide hypomethylation as well as hypermethylation of CPG islands is associated with tumor suppressor genes and developmental regulators and are characteristics of cancer cells changes in DNA methylation patterns associated with carcinogenesis progression gradually with the cell proliferation. CPG island methylation primarily targets promoters characterized by low gene expression. DNA methylation is a chemical modification that defines cell type and line lineage through the control of gene expression and genome stability. Disruption to the patterns of DNA methylation control mechanisms that are contributed to a bunch of diseases, especially cancer. Cancer cells are characterized by a barrant methylation such as genome-wide hypomethylation, and site-specific CPG hypermethylation, mainly targeting those CPG islands in gene expression regulatory elements. In particular, the early findings that a variety of tumor suppressor genes are target of DNA Hypermethylation in cancer has led to the proposal of a model in which a Barr DNA methylation promotes cellular oncogenesis through tumor suppressor gene silencing.
The cancer genome atlas, which I referred to earlier in this talk, is a comprehensive and coordinated effort to accelerate our understanding of the molecular basis of cancer through the application of genome analysis technologies, including large scale genome sequencing. The collaborative effort of the cancer Genome Atlas program advances personalized medicine.
When we analyze our subset of genes identified by the cancer genome atlas and shared publicly that are differentially expressed in patients with breast cancer and high mammographic density, we then uploaded our methylation gene list to a bioinformatic platform known as David to help identify any enriched themes in um, biological functionality for the subset of our genes. The David platform is the database for annotation visualization and integrated discovery and provides a comprehensive set of functional annotation tools for investigators to understand the biological meaning behind some of the large gene lists, such as the one that we isolated for our mammographically dense and our non mammographically dense patients. The star on the slide indicates pathways that are currently under validation in our lab and the hashtag indicates publications that have already been accepted for our gene analysis. That list.
This slide (R) shows a subset of genes that are both downregulated transcription repressed and methylated from our large subset of genes, which included the 749 probes found in the MoMA data. Also highlighted on this slide are two of the genes which we found upregulated in our dataset that have gone on for further functional analysis in our lab analysis of a selection of genes up upregulated in breast cancer and associated with epithelial to mesenchymal transition or EMT was performed utilizing the cancer genome atlas set and the database for functional annotation visualization and integrated discovery. Using the DAVID platform for pathway analysis, our results indicated an upregulation of two genes, tumor necrosis factor alpha in mammographically dense and non mammographically dense breast cancer cells, and the upregulation of zinc finger ebox binding protein one or ZEB one only. In the mammographically dense cells, TNF alpha is a pro-inflammatory cytokine and ZEB one is a transcription factor which directly affects the chromatin. We know that ZEB one regulates e deering expression and is a major cell to Sian protein and known to be a tumor suppressor protein in some cancers. Downregulation of eide and primes the detachment of cancer cells increases migration and invasion as well as metsis. Because of the crucial role of ZB one in this derrin regulation, ZEB one is considered a key regulated of EMT and tumor metastasis.
Our studies have shown that gene expression upregulation of these two key genes, ZB one and TNF Alpha, also induced functional changes in our cell lines, which include cellular proliferation and invasion. Being that TNF alpha and ZB one promote cell displacement and invasive myth through that EMT pathway, we hear and propose that these genes employ a pathogenic mechanism to render mammographically dense cells to metastasize. EMT is an overly complex but also reversible event. Therefore, further investigation into these genes in the an inhibition of either TNF alpha or Zev one might be an effective strategy for personalized medicine and cancer therapy.
Breast cancer tumors consist not only of tumor cell and cancer stem cells, but contain other cells within the tumor promoting functions such as cancer associated fibroblasts, normal fibroblasts myofibroblasts, mesenchymal stem cells, tumor associated adipocytes, endothelial cells, and various immune cells. These could include macrophages, neutrophils, natural killer cells, and regulatory T cells. We are currently in the process of further functional validation of our subset of genes and utilization of our three D cell culture model to model dense breast tissue in women Translational relevance.
Mammographic density is the strongest risk factor for nonfamilial breast cancer among women apart from older age, but its mechanistic underpinnings are poorly understood. We hypothesize that mammographic density would be associated with different subtypes of breast cancer based on their defining molecular pathways. Some of those pathways have be, have been delineated in our functional analysis study. Our results show that these well-defined molecular subtypes of normal tissue are strongly associated with both mammographic density and breast tissue composition, establishing novel molecular correlations of mammographic density to our gene expression analysis.
Many of the pathways enriched in patients such as epithelial to mesenchymal transition with higher mammographic density are certainly targetable raising the possibility of developing prevention strategies for mitigating density associated breast cancer risk. Future work in the lab will include clinical analysis with the Bard Cancer Center to validate some of our in vitro findings through both our expression array data, our gene subset, as well as our three dimensional cell culture analysis. We will continue to validate the three D cell culture model as well as confirm some of the genetic changes and epigenetic changes that we have already seen in our subset of gene. We plan to do further functional analysis to test the validated candidates and then provide a platform where we can undergo a personalized medicine approach using targeted therapeutic approaches.
Material Disclosure: Except as expressly set forth herein, as between the Parties, each Party is and shall remain the owner of all intellectual property that it owns or controls as of the effective date 11/1/2023 or that it develops or acquires thereafter. This information including all images and statements presented herein are submitted under limited license and are copyrights held and maintained by the speakers/producers of each segment and are protected under U.S. and international copyright laws adhering all intellectual properties. All content and intended solely for the attention and use of the recipient of the email with which this document is attached. This information is protected by work product privilege or other legal rules. It must not be disclosed to any person without our authority or published, posted or shared to other parties unknown in any way.
WOMEN’S HEALTH COLLABORATIVE GOES TO ALBANY
May 21, 2024, leading members of the NY Cancer Resource Alliance (NYCRA) held a special meeting with State Senator Patricia Canzoneri‐Fitzpatrick (of Senate District 9) to discuss critical issues associated with women's cancers. This initial meeting of the minds offered cancer updates from the field, including statistics, diagnostic trends and the continuing battle with restrictive insurance coverage.
Friday, May 10, 2024
NEWS RELEASE: The National Coalition for Ultrasound Screening
5/1/2024- The Women’s Health Collaborative (WHC) officially launches what educational director Dr. Roberta Kline calls “the ultimate alliance of women’s health champions”. This united volunteer group consists of public resources for women’s cancer, dense breast advocacy, research foundations of complex disorders (ie. Endometriosis and pelvic floor issues) and medical specialists from the private sector. This coalition aligns the promotion of ultrasound technology as the common life-saving solution for affordable and effective medical screening programs.
FOR IMMEDIATE RELEASE
The 2024 Women's Health Resource Network Launches Ultrasound Screening Initiative for Underserved Communities
In support of the underserved and underdiagnosed women, the WHC was originally founded to bring early detection and public education about the many women’s health disorders that many find to be lacking in access and information. This doctrine united women’s health advocates like Geri Barish (Hewlett House), Joe Cappello (co-founder of the Are You Dense? Foundation), Dr. Robert Bard (IHRC / Integrative Health Research Center), Dr. Noelle Cutter (Molloy University Research on Ovarian and Breast Cancer research programs) and Nancy Novack (of nancyslist.org). “It’s time we wake up lawmakers and the medical community to re-evaluate the existing gold standards (like mammography),” stated Mr. Cappello during a Key to the City speech honored by Waterbury mayor Neil O’Leary. “We are finally picking up great steam in our national push to have all clinicians adopt the advanced results of ultrasound technology… as a sustainable and affordable solution for ALL women!”
In a recent “Cancer Powermeet” event, leading advocacy leader Ms. Barish joined the WHC concept about “EARLIER DETECTION” in support of proactive screenings for women from 20-39. “Due to the continuing rise in numbers of breast cancer cases in younger women, doctors need to change their thinking about starting checkups at 40.” Innovative screening plans comprise the use of ultrasound in screening centers and traveling vans as a starting point in underserved locations. For over 20 years, Ms. Barish has been active in state congress about a list of cancer related interests impacting women’s health including public initiatives like environmental causes and legislative change in healthcare protocols.
THE NON-INVASIVE MOVEMENT
Cancer Imaging specialist Dr. Robert Bard presented a lecture in the 2024 Ultracon (AIUM) Symposium about diagnostic and screening innovations advancements the next stage in women’s longevity. “In the 1990's, 3D imaging allowed us to accurately detect uterine cancer, and particularly see abnormal ovarian tumors. In addition, imaging allowed us to detect an entire classification of ovarian cysts. Where ovarian cancer was once known as the ‘silent disease”, today's 3D ultrasound imaging brought the battle lines forward … as it can now identify potentially cancerous tumors in the glands in earlier stages pre-metastases. Creating a coalition promoting new education and clinical application of ultrasound is a game-changer-- offering a most affordable and highly accessible real-time scanning for immediate answers for women’s concerns”.
The outreach team behind the WHC aims to connect with lawmakers and health professionals alike, in pursuit of change through awareness. The Women’s Health Collaborative continues its mission to unite with new resources in support of better screening, community outreach and educational efforts to improve healthcare for women.
"In order to catch cancer, you need to be able to detect it at an early stage so we can treat patients with the most effective mechanisms. Ultrasounds are an easy, cost-effective method for screening for early breast cancers, especially in women below the age of 45, who are likely to have dense breasts. When you are young and premenopausal your breasts are dense and we know that breast density is linked to cancer and which also makes it harder for cancers to be seen on a mammogram. Although breast cancer is rare in women under the age of 40, early detection is key. Public health campaigns are spending so much money on mammograms for this population of women who can easily and cost effectively be screened using an ultrasound." - By: Noelle Cutter, PhD
PROGRAM 1: EARLIER DETECTION
27 YEAR OLD STAGE3 BREAST CANCER VICTIM SURVIVED - DESPITE OF DOCS WHO MISDIAGNOSED!In the year 2015, I was diagnosed with a stage three breast cancer on my right breast. It was a triple negative. When I did my own research, it just really means it tested negative on three aspects of tests with (I believe) estrogen. I feel if I didn't follow my intuition or demand answers (since I found this lump), I wouldn't be here today because records have shown when we're younger, they don't really take it as seriously. I would say be your own advocate! Get the answers you deserve because there is always a cause. If you have a lump, obviously there is a cause for it. So even if they tell you otherwise, keep asking and keep digging for answers. Find out the cause of this lump and more importantly, find out what it really is! (See full report | Video)
Tuesday, September 19, 2023
A NEED TO STANDARDIZE SCREENING WITH DENSE BREAST SCANNING
RUNNING THE TORCH OF A DENSE BREAST CANCER CHAMPION
Dr. Noelle Cutter drives the spirit of Dr. Nancy Cappello's mission for early cancer detection for women with dense breasts alongside Dr. Robert Bard's dense breast screening pilot program (8/27-29) - and the global pursuit to expand current screening standards.
A mammogram shows how dense your breasts are. When you get the results of your mammogram, you may also be told if your breasts have low or high density. Women with dense breasts have a higher risk of getting breast cancer.
PARTS OF THE BREAST
A woman’s breast has three kinds of tissue: FIBROUS TISSUE holds the breast tissue in place. GLANDULAR TISSUE is the part of the breast that makes milk, called the lobes, and the tubes that carry milk to the nipple, called ducts. Together, fibrous and glandular tissue are called fibroglandular tissue. FATTY TISSUE fills the space between the fibrous tissue, lobes, and ducts. It gives the breasts their size and shape.
BREAST CANCER RISK: Women with dense breasts have a higher chance of getting breast cancer. The more dense your breasts are, the higher your risk. Scientists don’t know for sure why this is true. Breast cancer patients who have dense breasts are not more likely to die from breast cancer than patients with non-dense (fatty) breasts.
7/8/2021- A wave of recognized medical sites, journals and reports are now indicating that dense breast tissue increases the risk of developing breast cancer and often masks a tumor from being seen on the mammogram since dense tissue is white and cancerous tissue is also white. Mammograms are the standard screening test for breast cancer, however, in the 21st Century, ultrasound non invasive imaging is the preferred exam for dense “lumpy” mammary disease.
The 1st World Conference of Breast Ultrasound in Philadelphia (1979) recognized ultrasound superiority in dense breast diagnostics but the density level was never quantified until recently. Mammography assessment of breast density is graded into four categories. Mammographers readily admit that these levels are subjective at best and technical factors such as mammary tissue compression and x-ray voltage/amperage dramatically influence the darkness or whiteness of the image.
Tuesday, September 28, 2021
Dense Breast Research: Code name IRON-WOMAN
Research overview: MAMMOGRAPHIC DENSITY, PHYSICAL ACTIVITY AND BREAST CANCER
Written by: Dr. Noelle Cutter / Sept. 12, 2021 Edited by: the publishing team @ NYCRANEWS.com
Mammography, as the primary screening modality, has facilitated a substantial decrease in breast cancer-related mortality in the general population. However, the sensitivity of mammography for breast cancer detection is decreased in women with higher breast densities, which is an independent risk factor for breast cancer. With increasing public awareness of the implications of a high breast density, there is an increasing demand for supplemental screening in these patients. Yet, improvements in breast cancer detection with supplemental screening methods come at the expense of increased false-positives, recall rates, patient anxiety, and costs. Therefore, breast cancer screening practice must change from a general one-size-fits-all approach to a more personalized, risk-based one that is tailored to the individual woman's risk, personal beliefs, and preferences, while accounting for cost, potential harm, and benefits.
FACTOIDS & FIGURES- The Inspiration behind our research initiative [1]:
▪ Breast cancer is the second most common cancer among women in the United States and about 1 in 8 U.S. women (about 13%) will develop invasive breast cancer over the course of her lifetime.
▪ In 2021, it is estimated that over 280,000 new cases of invasive breast cancer will be diagnosed in women in the U.S.,
▪ Over 40,000 women in the U.S. are expected to die in 2021 from breast cancer. Unfortunately, death rates have been steady in women under 50 since 2007, despite advancements in treatment options.
▪ For women in the U.S., breast cancer death rates are higher than those for any other cancer, besides lung cancer.
▪ As of January 2021, there are more than 3.8 million women with a history of breast cancer in the U.S. This includes women currently being treated and women who have finished treatment.
▪ Breast cancer is the most commonly diagnosed cancer among American women. In 2021, it's estimated that about 30% of newly diagnosed cancers in women will be breast cancers.
▪ Breast cancer became the most common cancer globally as of 2021, accounting for 12% of all new annual cancer cases worldwide, according to the World Health Organization.
▪ A woman’s risk of breast cancer nearly doubles if she has a first-degree relative (mother, sister, daughter) who has been diagnosed with breast cancer.
▪ About 5-10% of breast cancers can be linked to known gene mutations inherited from one’s mother or father. Mutations in the BRCA1 and BRCA2genes are the most common. On average, women with a BRCA1 mutation have up to a 72% lifetime risk of developing breast cancer. For women with a BRCA2 mutation, the risk is 69%. Breast cancer that is positive for the BRCA1 or BRCA2 mutations tends to develop more often in younger women.
▪ About 85% of breast cancers occur in women who have no family history of breast cancer.
The most significant risk factors for breast cancer are sex (being a woman) and age. But recent research is beginning to clarify additional risk factors associate with BC
PHYSICAL ACTIVITY Physical activity is considered a significant modifiable factor in breast cancer risk, and since exercise reduces fatty tissue and BMI, it has been thought to increase breast density. However, studies into the relationship between physical activity and breast density have been inconclusive. Other factors such as alteration in metabolism of endogenous hormones, are suggested to influence mammographic density (MD) as well. Therefore, it is evident that the links between physical activity and breast cancer risk need to be clarified.
BREAST TISSUE DENSITY Breast density levels refer to the appearance of the breast tissue on a mammogram. Breast density is part of the supportive or connective tissue that makes up the breast tissue. As you can see in this image, breast tissue is white to gray and transparent against a dark background. Denser breast tissue appears more white whereas fatty/non-dense tissue appears grapy and transparent.
Levels of density are described using a results reporting system called Breast Imaging Reporting and Data System (BI-RADS). The levels of density are often recorded in your mammogram report using letters. The levels of density are:
A: Almost entirely fatty indicates that the breasts are almost entirely composed of fat. About 1 in 10 women has this result.
B: Scattered areas of fibroglandular density indicates there are some scattered areas of density, but the majority of the breast tissue is non-dense. About 4 in 10 women have this result.
C: Heterogeneously dense indicates that there are some areas of non-dense tissue, but that the majority of the breast tissue is dense. About 4 in 10 women have this result.
D: Extremely dense indicates that nearly all of the breast tissue is dense. About 1 in 10 women has this result.
In general, women with breasts that are classified as heterogeneously dense or extremely dense are considered to have dense breasts. Almost half of women undergoing mammograms have dense breasts.
FATTY TISSUE vs. DENSE TISSUE A close up here shows the difference in imaging for a breast tumor on non-dense vs dense breast tissue using a mammogram. Breast density has been widely considered a strong risk factor for breast cancer, with statistics suggesting as much as a six times higher likelihood of the disease in breasts, compared with those with a less dense breast tissue. Not only does dense breast tissue make it harder for a mammogram to pick up small tumors, but dense breasts themselves have been associated with a higher chance of cellular abnormality.
WHY IT MATTERS? Women who have dense breast tissue have a higher risk of breast cancer compared to women with less dense breast tissue. It’s unclear at this time why dense breast tissue is linked to a higher lifetime risk of breast cancer. Understanding that link is extremely important.
Dense breast tissue also makes it harder for radiologists to see cancer. On mammograms, dense breast tissue looks white. Breast masses or tumors also look white, so the dense tissue can hide tumors. But fatty tissue looks almost black. On a black background it’s easier to see a tumor that looks white. So, mammograms can be less accurate in women with dense breasts.
One of the challenges in promoting the widespread utility of breast cancer risk prediction models has been the assertion that most women with a diagnosis of breast cancer have no established clinical breast cancer risk factors or are not considered to be high risk. [1][2] Although it is impossible to determine the cause of breast cancer in any individual case [3] easily assessed risk factors that explain a substantial proportion of incident breast cancers can be used to stratify breast cancer risk for targeted screening [4] and primary prevention [5] and improve public health interventions to reduce breast cancer risk.
Recent research has suggested that for women with dense breasts, a screening strategy that also takes into account a woman’s risk factors and protective factors may be the best predictor of whether a woman will develop breast cancer after a normal mammogram and before her next scheduled mammogram.
MAMMOGRAPHIC DENSITY Breasts contain glandular, connective, and fat tissue. Breast density is a term that describes the relative amount of these different types of breast tissue as seen on a mammogram. Dense breasts have relatively high amounts of glandular tissue and fibrous connective tissue and relatively low amounts of fatty breast tissue.
HOW COMMON ARE DENSE BREASTS? Nearly half of all women age 40 and older who get mammograms are found to have dense breasts. Breast density is often inherited, but other factors can influence it. Factors associated with lower breast density include increasing age, having children, and using tamoxifen. Factors associated with higher breast density include using postmenopausal hormone replacement therapy and having a low body mass index.
Women with dense breasts have a higher risk of breast cancer than women with fatty breasts, and the risk increases with increasing breast density. This increased risk is separate from the effect of dense breasts on the ability to read a mammogram. MD one of the strongest risk factors. And because individuals with denser breasts tend to develop more serious types of breast cancer, understanding the connection is important.
ATHLETES A common question that invariably comes up when discussing breast density relates to breast density in athletes. As an athlete myself who has dense breasts, I was struck by the number of individuals in my athletic community who also have dense breasts. A shocking trend was seen in the overwhelming amount of young women with dense breasts who subsequently had received false negative mammogram reports.
What we do know is that your breast tissue tends to become less dense as you age, though some women may have dense breast tissue at any age. Women with less body fat are more likely to have more dense breast tissue compared with women who are obese. From observation (thus far), athletic women are also more likely to have dense breast tissue. One of the main goals of our study is to really try to understand the biological connection of breast density in athletes as well as run a retrospective study on how common this trend is.
RESEARCH OBJECTIVES It's not clear why some women have a lot of dense breast tissue and others do not. You may be more likely to have dense breasts if you:
▪ ARE YOUNGER; your breast tissue tends to become less dense as you age, though some women may have dense breast tissue at any age.
▪ HAVE LOWER BMI (body mass index); women with less body fat are more likely to have more dense breast tissue compared with women who are obese.
Breast density is shown to be associated with breast cancer risk in women aged 40 to 65 years, but there is limited evidence thus far of its association with risk of breast cancer among women 18+. Furthermore, a high proportion of women with low BMI present with dense breasts, making them likely candidates to receive false negative readings on a mammogram. We aimed to estimate the proportion of breast cancers attributable to breast cancer risk factors commonly documented in clinical practice and used in breast cancer risk prediction models, including BI-RADS breast density and ultrasounds to confirm mammography readings. Our data will be collected from a cohort of women undergoing ultrasound density scans at the Bard Cancer Center (NYC).
Although breast density is a well-established, strong, and prevalent breast cancer risk factor it’s biological connection is not clearly understood. More research is needed to support the population associated risk proportion in athletic pre-menoposal women. Our data will start with a cohort of women undergoing imaging ultrasounds at the Bard Cancer Diagnostic Center. Our population will include pre-menoposal women with dense breasts.
METHODS Endurance athletes are defined those who participated in one or more endurance events (long course) in the year or as well as those who are (younger, low BMI cohort). MD and classification of “dense breasts” was heterogeneous and extremely dense as noted by the BI_RADS code; (heterogeneously or extremely dense vs scattered fibroglandular densities). Data will be collected as odds ratio (OR’s) and 95% confidence intervals included in our outcomes
Cross-sectional Analysis
1000+ pre-menopausal women aged 18+
Collect information on height, weight, BMI and history of disease
Physical activity assessment
MD measurement performed by radiologist and confirmed by ultrasound
Logistic regression used to estimate the association of MD within participation in physical activity
JAMA STUDY: A recent report in Journal of the American Medical Association found that first-degree family history of breast cancer dense breasts were associated with an increased population associated risk proportion of breast cancer. Among premenopausal women, the largest individual population associated risk proportion was for breast density, with 28.9% (95% CI, 25.3%-32.5%) of breast cancers potentially removed by reducing breast density from BI-RADS heterogeneously or extremely dense breasts to scattered fibroglandular densities. The population associated risk proportion for breast density increased to 65.5% (95% CI, 60.4%-70.6%) if all premenopausal women reduced their breast density to the lowest category of almost entirely fat tissue.
SUMMARY/ WRAP-UP Given that greater breast density as categorized by the BI-RADS remains a factor associated with breast cancer for all ages of women, information about breast density together with life expectancy may benefit clinical decision-making regarding screening. In March 2019, the US Food and Drug Administration recommended changes to the Mammography Quality Standards Act to make it mandatory to report breast density information to both patients and their physicians. However, how women and their physicians should use this information to inform screening recommendations is unclear. Very dense breasts may increase the risk that cancer won't be detected on a mammogram.
What is clear is that additional research is needed to elucidate the mechanisms underlying the observed associations between breast density and risk of breast cancer. As newer and more advanced breast density assessment techniques are developed, evaluation of the diffusion of such innovations with an aim of developing individualized screening strategies will be important, particularly among athletic women, for whom dense breast are more likely seen.
EPILOGUE
Dr. Noelle Cutter is a professor of biology, ironman finisher, and advocate for dense breast screening. United with an expanding research team dedicated to collecting data on women with dense breasts and screening options for these patients, her initiative aims to investigate and gather conclusive information about dense breasts in specific groups- including age, body mass index, and amount of physical activity and the underlying diagnostics of breast cancer tumors. This research program is under a partnership with Molloy College and Dr. Robert Bard, expert diagnostic cancer imaging specialist in NYC and other colleagues from the NY Cancer Resource Alliance.
With your support, we are able to implement this screening program for women's health as well as help fund this clinical research. Our work will advance technology, change legislation and most importantly save lives through awareness.
Wednesday, July 7, 2021
Ultrasound Significantly Reduces False Readings of DENSE BREASTS
Dr. Noelle Cutter drives the spirit of Dr. Nancy Cappello's mission for early cancer detection for women with dense breasts alongside Dr. Robert Bard's dense breast screening pilot program (8/27-29) - and the global pursuit to expand current screening standards.
A mammogram shows how dense your breasts are. When you get the results of your mammogram, you may also be told if your breasts have low or high density. Women with dense breasts have a higher risk of getting breast cancer.
PARTS OF THE BREAST
A woman’s breast has three kinds of tissue: FIBROUS TISSUE holds the breast tissue in place. GLANDULAR TISSUE is the part of the breast that makes milk, called the lobes, and the tubes that carry milk to the nipple, called ducts. Together, fibrous and glandular tissue are called fibroglandular tissue. FATTY TISSUE fills the space between the fibrous tissue, lobes, and ducts. It gives the breasts their size and shape.
BREAST CANCER RISK: Women with dense breasts have a higher chance of getting breast cancer. The more dense your breasts are, the higher your risk. Scientists don’t know for sure why this is true. Breast cancer patients who have dense breasts are not more likely to die from breast cancer than patients with non-dense (fatty) breasts.
Sunday, January 2, 2022
News Release: 2022 Research Trial- Dense Breast Detection
NY Cancer Alliance to Launch the First Dense Breast Research Study for Low BMI and Underserved Subjects
1/11/2022- Dr. Noelle Cutter (Biology professor and clinical researcher from Molloy College) joined with Dr. Robert L. Bard (top NYC radiologist and cancer diagnostic expert) to deploy the 2022 field study to provide breast screening to younger women, subjects with LOW BMI and those in underserved areas. "Through supplemental imaging (ie. 3D Doppler Ultrasound), we can provide better detection of tumors in dense breasts that are concealed by dense breast tissue from mammography."
Mammography is the current standard for breast cancer early detection for women 40 & older. Recent studies have shown nearly half of all women who get mammograms are found to have dense breasts, exposing this population to the risk that mammograms may miss potentially cancerous tumors concealed by dense breast tissue. Dr. Cutter's initial concepts to target LOW BMI (bet 12-22% body fat) was personally inspired. As an active TRIATHLETE, her own diagnosis sparked her survey and inquiry throughout the athletic community where she uncovered a significant trend that became the basis for this research. She wishes to target younger women, athletes and members of underserved communities. "Younger women may be more likely to have dense breasts... also I find athletes with LOWER BMI (body mass index) or those with less body fat are more likely to have more dense breast tissue compared with women who are obese."
Breast density is shown to be associated with breast cancer risk in women aged 40 to 65 years, but there is limited evidence thus far of its association with risk of breast cancer among women 18+ (mostly because mammography starts at 35 or 40). Furthermore, a high proportion of women with low BMI present with dense breasts, making them likely candidates to receive false negative readings on a mammogram. "We aimed to estimate the proportion of breast cancers attributable to breast cancer risk factors commonly documented in clinical practice and used in breast cancer risk prediction models, including BI-RADS breast density and ultrasounds to confirm mammography readings", states Dr. Bard.
Thanks to the digital (Web-shareable) platform of ultrasound, collaborating between multiple scanning locations allows all data to be collected and interpreted by Dr. Bard in his NYC clinical facility. "This allows us to have more scanning partners throughout the state and hopefully even across the country", says Joe Cappello, national patient advocate of AreYouDense.org.
The national expansion program of this screening pilot and remote-location training are supported by an expanding list of clinical and technological leaders in diagnostic imaging. "We are honored to join this research and educational crusade to save lives... where Ultrasound Imaging can perform such a vital role in uncovering so many cancer concerns more efficiently", states Alice Chiang, CEO or Terason Inc. The coordinated research team aspires to collect enough data from these demographic target groups (18+, low bmi and underserved women) to support the emphasis of dense breast concerns in our cancer detection community and the importance of supplemental scanning for all early detection facilities.
CANCER SPEAKER SERIES ON EARLY DETECTION & PREVENTION: FIGHTING CANCER THROUGH PUBLIC EDUCATION
NYCRA is a volunteer union of caregivers, educators, clinical professionals and survivors-turned-crusaders. One of our most powerful tools to help victims fight (and beat) cancer is AWARENESS. The medical partners and public advocates of NYCRA in conjunction with Awareness for a Cure and a list of cancer foundations offers some of the most enlightening and compassionate volunteer speakers to conduct presentations about public health awareness to bring comprehensive cancer education to large community groups & private orgs. We have some of the most recognized and dynamic coaches and speakers dedicated to bringing better understanding about cancer to all New Yorkers. Our seminars cover a wide variety of useful topics, current statistics, resources and the latest innovations. For more info. on our traveling speaker series or to inquire about booking an event, contact us at: nycralliance1@gmail.com















.webp)